Mind & Mystery · Sleep Science
Frozen in the Dark
When the mind wakes but the body refuses — the terrifying truth behind sleep paralysis
You open your eyes. The room is familiar, yet something is deeply, profoundly wrong. Your body will not move. Not a finger. Not an eyelid. A crushing weight presses on your chest, and at the edge of your vision — or perhaps right beside you — something watches. You cannot scream. You cannot run. You are, for these terrifying moments, a prisoner in your own flesh.
This is sleep paralysis — a phenomenon that has haunted human beings across every culture and every century, wearing a thousand different disguises: demon, ghost, old hag, shadow figure. Today, science gives it a name. But even scientists admit the experience remains profoundly, stubbornly strange.
What Exactly Is Sleep Paralysis?
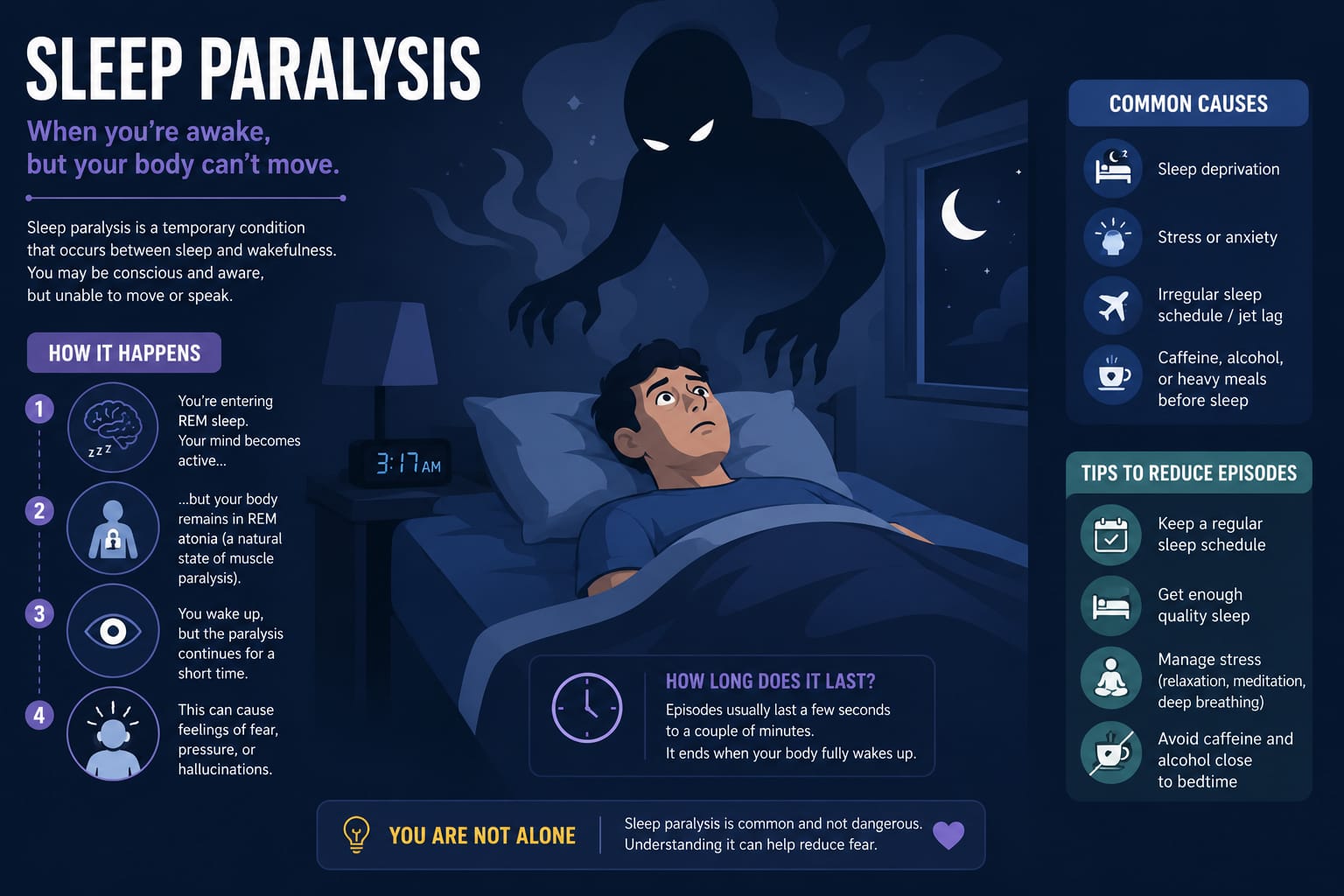
Sleep paralysis is a temporary state in which a person is conscious but completely unable to move or speak. It occurs at the boundary between wakefulness and sleep — most commonly just as you are falling asleep (hypnagogic paralysis) or just as you are waking up (hypnopompic paralysis).
During REM (Rapid Eye Movement) sleep, the brain essentially disconnects the body’s voluntary muscles to prevent you from physically acting out your dreams — a mechanism called REM atonia. Sleep paralysis happens when this muscle paralysis lingers as the mind begins to wake, creating a terrifying gap where awareness returns but control does not. Episodes typically last between a few seconds and two minutes, though to the person experiencing them, they can feel eternal.
Symptoms: More Than Just Stillness
Sleep paralysis is not merely the inability to move. It arrives with a constellation of deeply unsettling sensations that explain why it has terrified humans for millennia:
- Complete inability to move limbs or speak
- Intense pressure or weight on the chest
- Difficulty breathing or sensation of choking
- Vivid hallucinations — visual, auditory, or tactile
- Sense of a threatening presence in the room
- Intense fear, panic, or dread
- Feeling of floating or leaving the body
- Rapid heartbeat and shallow breathing
- Buzzing, humming, or whispering sounds
- Sensation of being touched or grabbed
The hallucinations are particularly striking. Researchers classify them into three types: the intruder (a threatening figure in the room), the incubus (a crushing entity on the chest), and vestibular-motor hallucinations (feelings of flying or falling). These are not vague impressions — they are photorealistic, sensory experiences indistinguishable from reality.
“The mind is awake, the body is asleep, and something in between manufactures pure, convincing terror.”
Strange Facts You Never Knew
- It’s surprisingly common. Studies estimate that roughly 8% of people experience sleep paralysis at least once — but in students and psychiatric patients, that number climbs as high as 28–32%.
- You can’t suffocate. Despite the crushing chest sensation, the body continues to breathe automatically. The sensation of choking is a hallucination generated by the brain.
- The “Old Hag” is universal. Across cultures that have had no contact with each other — from medieval Europe to Inuit communities — the same hallucination appears: an old, malevolent woman sitting on the sleeper’s chest.
- Astronauts may be more vulnerable. Disrupted sleep schedules, stress, and irregular environments — common in space — are all known triggers for sleep paralysis episodes.
- Lucid dreamers get it more often. People who practice lucid dreaming — consciously controlling their dreams — report significantly higher rates of sleep paralysis, as both involve unusual awareness during REM sleep.
- You can train yourself to end it. Sleep researchers suggest making small, deliberate movements — like wiggling a single toe — to gradually signal the brain to restore motor control and end the episode.
The Devil’s Work: Sleep Paralysis Through History
Long before neuroscience gave us the language of REM atonia, human beings experienced sleep paralysis and reached for the only explanations available to them — and those explanations were almost always supernatural.
In medieval Europe, the condition was attributed to the succubus or incubus — demons that would visit sleepers in the night, sitting upon their bodies and stealing their breath or violating them in their helpless state. The Church took these accounts with deadly seriousness. Women who reported such visitations were sometimes accused of inviting demonic contact, with consequences that could include trial, torture, or execution during the witch-hunt era of the 15th through 17th centuries.

In West Africa and the Caribbean, a similar phenomenon is known as “kokma” — the ghost of a dead baby that jumps on sleepers and throttles them. In Japan, the word “kanashibari” literally means “bound in metal” — the sensation of being held down by an invisible supernatural force. In Newfoundland, the “Old Hag” rides sleepers in the night; in Turkey, a cin (jinn) sits upon the chest of those it has targeted.
Even as recently as the 20th century, rural communities in parts of India, the Middle East, and Eastern Europe treated sleep paralysis episodes as evidence of spirit possession requiring exorcism, prayer, or ritual cleansing. Priests, shamans, and healers were called to the bedsides of those afflicted, performing elaborate ceremonies to drive out whatever had taken hold of the helpless sleeper’s body.
It was not until the 19th century that Western medicine began cataloguing sleep paralysis as a physiological phenomenon. The Dutch physician Isbrand van Diemerbroeck published an early description in 1664, and by the early 20th century, neurologists had begun connecting the experience to disruptions in the sleep cycle — though a full scientific understanding would not emerge until the discovery of REM sleep in 1953.
Who Is at Risk — and What Can Be Done?
Sleep paralysis is more likely to occur when the sleep-wake cycle is disrupted. Common triggers include irregular sleep schedules, chronic sleep deprivation, sleeping on one’s back, extreme stress or anxiety, and certain medications such as antidepressants. Narcolepsy — a neurological disorder affecting sleep regulation — is also closely associated with frequent sleep paralysis episodes.
The good news: for most people, sleep paralysis is an isolated event with no lasting harm. Maintaining a consistent sleep schedule, reducing stress, and avoiding sleeping in a supine position can significantly reduce its frequency. For those with recurring episodes, cognitive behavioural therapy and, in some cases, low-dose antidepressants prescribed by a physician have shown effectiveness.
Perhaps most reassuringly, understanding what sleep paralysis actually is — a glitch in the brain’s transition between states, nothing more — tends to dramatically reduce the terror it causes. The demon on your chest, it turns out, is just your own sleeping brain catching up with your waking mind.
“The same experience that once filled people with dread and sent them to their priests now fills sleep researchers with fascination — and still has no complete explanation.”
Leave a Reply